Coronary Artery Disease or atherosclerotic coronary vascular disease is a leading cause of morbidity and mortality worldwide. The incidence of CAD is alarmingly increasing in developing countries, particularly in India. Besides conventional risk factors for CAD like Diabetes Mellitus, 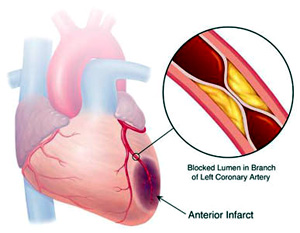 hypertension, dyslipidemia, smoking habits, positive family history, obesity and sedentary lifestyles, several emerging risk factors are also important for CAD incidence. These are lipoprotein a levels in blood, plasma homocysteine, hsCRP and probably genetic factors in Asian communities. There are several other newer risk factors for CAD among Asians but the casual relationship has not been clearly established. hypertension, dyslipidemia, smoking habits, positive family history, obesity and sedentary lifestyles, several emerging risk factors are also important for CAD incidence. These are lipoprotein a levels in blood, plasma homocysteine, hsCRP and probably genetic factors in Asian communities. There are several other newer risk factors for CAD among Asians but the casual relationship has not been clearly established.
The pathogenesis of CAD is the deposition of lipids in the subintimal region of the coronary arteries. This is also important for development of cerebral atherosclerosis, renovascular disease and peripheral arterial disease. The atherosclerotic process is the disease of ageing. It becomes evident from as early as 2 years of life and gradually progresses to become manifested at 4th or 5th decade of life. Females are generally protected until menopause because of the estrogenic effect which prevents deposition of fatty streaks in the arteries.
So the CAD remains asymptomatic for a long time. When an atherosclerotic plaque obstruct the arterial lumen > 70% of its diameter, then only the area will suffer from ischemia and symptoms will be evident. The symptoms of coronary ischemia is known as Ischemic Heart Disease 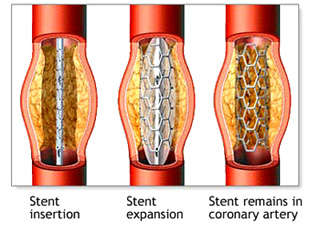 (IHD). It will become manifested only on exertion or excitement and will be relieved on rest. These is effort angina (stable CAD). (IHD). It will become manifested only on exertion or excitement and will be relieved on rest. These is effort angina (stable CAD).
Sometimes the endothelial lining the atherosclerotic plaque may become stable due to some or other reasons. The endothelium overlying the plaque may erode, ulcerate or rupture. These is a dangerous situation and is the cause of acute coronary syndrome. This disrupted endothelial lining will attract the platelets and coagulation cascade will be activated and rapid thrombus and platelet deposition will totally occlude the vessel. This is an emergency situation and should be tackled urgently preferably by urgent PCI. Why the plaque becomes stable is not definitely known but several factors like abnormal mental stress, fluctuation of BP, high levels of inflammatory markers like hs CRS and Homocysteine may play some role. The other presentations of CAD are arrhythmias, sudden cardiac death and heart failure.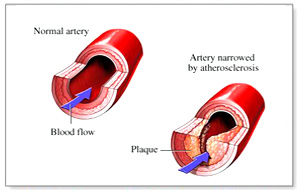
Whatever is the presentation, the treatment of CAD can be divided in three categories like medical therapy, coronary angiogram and PCI and CABG.
The medical therapy for CAD is indicated for stable CAD and for low risk unstable angina. In high risk unstable angina and acute MI the preferred mode of therapy is invasive like early CAG and PCI. Those cases where there is severe LM with triple vessel CAD and PCI is not feasible from technical ground, CABG will be considered. However complex PCI with multiple DES have equivalent result as per CABG in several trials. |

