 Homosexuality has been condemned by people most of the time; however homosexual behaviour has existed throughout history. In Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) it is mentioned under the heading of '302.9 Sexual Disorder Not Otherwise Specified' as 'Persistent and marked distress about sexual orientation'. Homosexual clients visit doctors for various reasons. Homosexuality has been condemned by people most of the time; however homosexual behaviour has existed throughout history. In Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) it is mentioned under the heading of '302.9 Sexual Disorder Not Otherwise Specified' as 'Persistent and marked distress about sexual orientation'. Homosexual clients visit doctors for various reasons.
- A young male person comes with erectile dysfunction. He is unmarried and anxious. He gives history of good sexual responses (including desire, erection, penetration and orgasm) with male partners. But has failed with females due to his selective erectile inadequacy. Upon detailed questioning he is found to be homosexual.
- Sometimes a young male is brought to doctor's clinic for assessment of his masculinity. He has allegedly failed to satisfy his wife sexually, who he has recently married. Their marriage has remained unconsummated. Wife says her husband is not at all interested in her. Male who is now facing marital breakdown and legal consequences reluctantly gives history of his homosexual interest and activities.
- Occasionally person comes with primary complaint of his homosexual tendencies. He feels embarrassed, ashamed and guilty of his own traits. He wants to get rid of his "bad habits".
- If clinicians cultivate habit of taking detail sexual history of all patients having sexually transmitted disease. HIV-AIDS and recurrent anorectal problems, he may find homosexual behaviour in some of these patients.
- Exceptionally, a homosexual may come, to sex therapist's clinic and ask for a list of his/other homosexual patients. Needless to say such client is never interested in treatment. They are in search of a partner.

THE MANAGEMENT OF PROBLEMS
Before treating homosexual clients one should always keep in mind that homosexuality is not considered as a disease. Only those individuals who are not comfortable with their own homosexuality and who wants to be heterosexual can be accepted for treatment. These homosexuals are known as ego-dystonic people. The remaining are ego-syntonic who enjoy their homosexuality comfortably and who never want to change themselves.
Managing homosexual patient is a difficult and tricky job. Clinician must be comfortable with his own sexuality. Outcome of any treatment modality is less than satisfactory. Clinician should ensure compassionate, warm and empathetic relationship. Clinicians' individual philosophical values should not be imposed upon that of their clients. Following are the few guidelines about the treatment of homosexual clients :
 Drugs including hormones have no role in management of homosexuality. Drugs including hormones have no role in management of homosexuality.- Gradual systematic desensitization is a kind of behavioural therapy which can be attempted in selected patients. Patients are taught to feel relaxed. In relaxed state of mind they are encouraged to have heterosexual fantasy. Simultaneous viewing of erotic photographs or films can be .helpful. Those bisexual patients who also have some interest in opposite sex can be benefitted. But results are unpredictable.
- Various psychodynamically and analytically oriented therapies are practised by trained psychotherapist in which meaning of homosexuality, motives, pattern of relationship and early experiences of life are explored.
- As most of the societies are still antihomosexual (homophobic) and as still
homosexuality is considered, crime, sin, nuisance, illness or antisocial
activity; they frequently become anxious, frustrated, depressed or even
suicidal. They have to hide their preferences. They constantly struggle in
marriage, family, friend circle, job and society.
They struggle with themselves, due attention must be paid to reduce these stresses, anxiolytics, antidepressants, antipsychotics can be prescribed judiciously if required. Marital counselling is must to reduce spouse frustration, anger, guilt or hostility. Family therapy is advocated in case of deteriorating family atmosphere highly charged emotional encounters.
- Erectile dysfunction can be handled with intracavernosal injections of vasodilators temporarily, sensate focus with mutual pleasuring can also be attempted side by side in selected patients, pharmacological management is especially rewarding in patients having unconsummated marriage.
 Some wives accept husband's homosexuality and still they would ask for children. Intravaginal ejaculation is required for procreation. Fertility is considered single most important goal for couple's successful marriage life. AIH can be tried out in case of refractory non-consummation. Some wives accept husband's homosexuality and still they would ask for children. Intravaginal ejaculation is required for procreation. Fertility is considered single most important goal for couple's successful marriage life. AIH can be tried out in case of refractory non-consummation.- In case of an egosyntonic homosexual, teaching how to perform safe sex should not be forgotten. Many homosexual males have multiple partners. Limiting the number of partners, proper use of condoms, fidelity and emotional bondage with same sex partner, care of anal tears and STDs etc. also constitute important part of their management.
- Female homosexuals,(lesbians) hardly present for treatment, same guidelines can be followed for them also.
- Adolescent boys sometimes are brought to the therapist. They have been caught red handed by their parents. Parent says that they indulge into 'dirty games' of touching genitals of other boys. Management of such events requires parental counselling. They must be reassured.
The way societies all over the world are becoming more and more open about homosexuals, the time may come when homosexuality will be totally accepted and they need not seek treatment for their emotional insecurities, inferiority and social maladjustment.
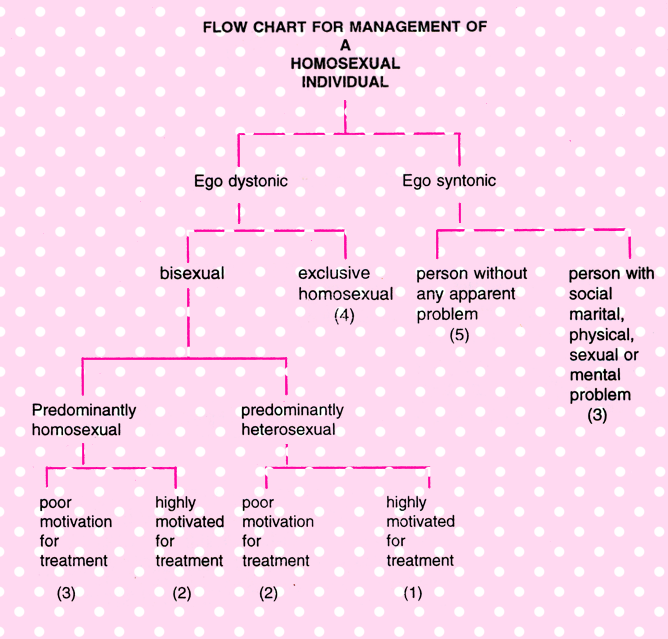
- Treatment should be attempted, outcome may be positive.
- Treatment may be attempted, outcome uncertain
- Treatment may be attempted, with less than satisfactory results
- Treatment possible with poor outcome.
- Treatment neither sought for, nor advisable.
|







