Fractures of the pelvis and a
cetabulum are among the most serious injuries treated by orthopedic surgeons. Often the result of a traumatic incident such as a motor vehicle accident or a bad fall, these fractures require rapid and precise treatment and, in some cases, one or more surgical procedures. People of all ages are vulnerable to these injuries. In addition, some elderly patients with fragile bones due to osteoporosis develop pelvic fractures and fractures of the acetabulum with a lower impact fall.
Radiograph of a normal pelvis The complex nature of these fractures can be better understood by looking at the anatomy that is involved. The pelvis is made up of several bones (ileum, ischium and pubic bones) which create a bony ring, meeting at the pubic symphysis in the front and the sacrum (a bone situated at the lower end of the spine) in the back. Together with a number of ligaments and muscles, the bones of the pelvis support the weight of the upper body and rest on the hip joints. The pelvis protects abdominal organs including the intestines and the bladder, as well as major nerves and blood vessels. Pelvic fractures may occur at any location on the bones depending on the nature of the accident and the areas of impact.
Radiograph of the pelvis demonstrating a fracture of the pubic bone
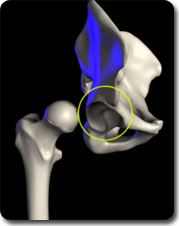
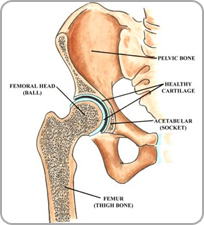
The acetabulum refers to the part of the pelvis that meets the upper end of the thigh bone (the femoral head) to form the hip joint. In a healthy hip, these two bones fit together like a ball and cup, in which the ball rotates freely in the cup. Cartilage lines the bones where they meet at the joint and there is little friction between the surfaces during movement.
Anatomical illustration of the acetabulum
The term broken hip usually refers to a fracture of the ball portion of this joint, that is, the upper femur, femoral neck or the femoral head. (See Hip Fracture for more on this injury.) In this section, we are speaking specifically of a fracture of the cup or acetabulum. Fractures of the acetabulum are harder to treat because access to this bone is more difficult, and because of the acetabulum's proximity to the major blood vessels to the legs, the sciatic nerve (the major nerve that arises from the lower spine and provides sensation and movement to the leg and foot), the intestines, the ureter and the bladder. Unlike a hip fracture, which can be treated relatively easily, to repair an acetabular fracture, the orthopedic surgeon, must, in essence, fix the broken bones from the inside out.
In fractures of this type, the femoral head is often driven through the acetabulum because of the impact of the fall or accident. If the femoral head ends up outside the acetabulum, this is known as a dislocation of the hip joint. Some patients have both a fracture and a dislocation.
Radiograph of the left hip demonstrating a posterior dislocation of the hip with an associated Posterior Wall type fracture of the acetabulum.
Unfortunately, patients with fractures of the pelvis and/or acetabulum, almost always also experience serious injury to surrounding soft tissue (skin and muscles) and neurovascular structures (nerves, arteries and veins). In addition, especially in the case of pelvic fractures, adjacent organs can be seriously injured. With both types of fracture, there is significant bleeding and risk of nerve damage.

In patients with multiple injuries, treatment begins with the trauma team at the scene, and then subsequently in the emergency room--a team of general surgeons, anesthesiologists and nurses--who work together to control bleeding, address damage to the head and chest, and other organs that may have been affected, such as the bladder and intestines, and to stabilize broken bones. During this early resuscitation phase of treatment, the orthopedic surgeon may need to stabilize the fracture by using an external frame to temporarily hold the bones in proper alignment while other problems are treated. This is called temporary external fixation. Surgeons construct these frames using steel pins that are inserted into the bone and joined together by clamps and rods and can do so very rapidly.
Radiograph of the pelvis demonstrating application of a pelvic external fixator.
Once the patient is stabilized--bleeding has stopped and other life-threatening injuries have been addressed--the fractures can be treated definitively. Successful treatment for both of these types of fractures requires the skills of an interdisciplinary team, with orthopedic surgeons working closely with the trauma team (general surgeons), the anesthesiologists and nurses. Following surgery, rehabilitation specialists play a key role in recovery.
Because of the complex nature of these fractures and because many orthopedic surgeons do not regularly treat them, patients who initially go to a community hospital for emergency attention are often transferred to an institution that specializes in such injuries.
