An arrhythmia is an irregular heartbeat - the heart may beat too fast (tachycardia), too slowly (bradycardia), too early (premature contraction) or too irregularly (fibrillation). Arrhythmias are heart-rhythm problems - they occur when the electrical impulses to the heart that coordinate heartbeats are not working properly, making the heart beat too fast/slow or inconsistently.
Many heart arrhythmias are harmless. We all occasionally experience irregular heartbeats, which may feel like a racing heart or fluttering. Some arrhythmias, however, especially if they veer too far from a normal heartbeat or result from a weak or damaged heart, may cause troublesome and even potentially fatal symptoms.
Rapid arrhythmias are called tachycardias, while slow ones are called bradycardias. Irregular arrhythmias - when the heartbeat is irregular - are called fibrillations, as in atrial or ventricular fibrillation. When a single heartbeat occurs earlier than it should it is called premature contraction.
The English word "arrhythmia" comes from the Greek word rhymos, meaning "rhythm", the Greek suffix a (letter "a" added to the beginning of a word) means "loss" - put together they mean "loss of rhythm".
What are the signs and symptoms of arrhythmia?
Some patients may have no symptoms at all. A doctor may detect a sign of arrhythmia during a routine examination. (The patient detects/feels a symptom, and other people, such as the doctor or other members of the household, detect a sign).
Even if a patient notices symptoms, it does not necessarily mean there is a serious problem. Ironically, some patients with life-threatening arrhythmias may have no symptoms, while others with symptoms may not have a serious problem.
Symptoms of tachycardia include: (Sometimes there are no symptoms)
Breathlessness
Dizziness
Syncope (fainting, or near-fainting)
Fluttering in the chest
Lightheadedness
Sudden weakness
Symptoms of bradycardia include: (Sometimes there are no symptoms)
Angina (chest pain)
Concentration problems
Confusion
Difficulties when exercising
Dizziness
Fatigue (tiredness)
Lightheadedness
Palpitations
Shortness of breath
Syncope (fainting or near-fainting)
Symptoms for atrial fibrillation (these often develop rapidly): (Sometimes there are no symptoms)
Angina (chest pains)
Breathlessness
Dizziness
Palpitations
Syncope (fainting, or near-fainting)
Weakness
What are the causes of arrhythmia?
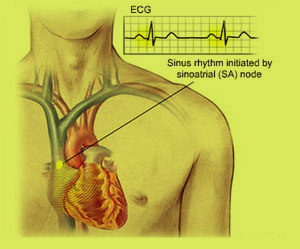
The electrical impulses that cause the heart to contract must follow a precise pathway for it to work properly. Any interruption to these impulses can result in arrhythmia. The human heart consists of four chambers - the chambers on each half of the heart form two adjoining pumps, with the atrium (upper chamber) and the ventricle (lower chamber).
When a heartbeat occurs the less muscular and smaller atria contract and fill the relaxed ventricles with blood. The contraction starts when a small group of cells in the right atrium (the sinus node) send an electrical impulse which causes the right and left atria to contract. The impulse then moves to the atrioventricular node (at the center of the heart) on the pathway between the atria and ventricles. From here the impulse leaves the atrioventricular node, travels through the ventricles, causing them to contract and pump blood - this blood pumps throughout the body.
For a person with a healthy heart the process works properly and he/she should have a heart rate of between 60 and 100 beats per minute when resting. The fitter you are the lower your resting heart rate. Olympic athletes, for example, will usually have a resting heart rate of less than 60 beats per minute because their hearts are very efficient.
What are the risk factors for arrhythmia?
Old age - the heart inevitably weakens as we get old and loses some of its flexibility - this affects the conduction of electrical impulses.
Inherited gene defects - people who are born with a heart abnormality have a higher risk of developing arrhythmia.
Heart problems - people with heart problems, narrowed arteries, those who have had a heart attack, heart valves that do not function properly, previous heart surgery, and cardiomyopathy, are more likely to develop arrhythmia.
Hypothyroidism or hyperthyroidism - people with a thyroid gland problem are more likely to develop arrhythmia.
Medications - some prescription medications, as well as OTC drugs, such as cough and cold drugs containing pseudoephedrine may help in the development of arrhythmia.
Hypertension - people with high blood pressure are much more likely to developcoronary artery disease and other heart problems which result in the improper conduction of electrical impulses.
Obesity - obesity is linked to a huge number of health problems, including diabetes type 2, cancer, cardiovascular disease, heart disease, and arrhythmia.
Uncontrolled diabetes - a patient with uncontrolled diabetes is significantly more likely to develop arrhythmia compared to a patient who has his diabetes under control (receives proper treatment).
Obstructive sleep apnea - patients with obstructive sleep apnea may experience bradycardia or atrial fibrillation more commonly than other people.
Electrolyte imbalances - electrolytes are essential for the proper conduction of electricity between cells and through cells. If electrolyte levels are wrong - either too low or too high - the electrical impulses in the heart may be affected, resulting in arrhythmia.
Heavy and regular alcohol consumption - people who regularly consume large quantities of alcohol are much more likely to develop atrial fibrillation.
Too much caffeine - caffeine, and some other stimulants, may accelerate the heart rate and eventually cause arrhythmias.
Illegal drugs - amphetamines and cocaine can cause arrhythmias, especially ventricular fibrillation.
What are the treatment options for arrhythmia?
Treatment for arrhythmia is only required if it is putting the patient at risk of a more serious arrhythmia or a complication.
Treatment for bradycardias (heartbeat is too slow)
If the bradycardia is caused by an underlying problem, such as an underactive thyroid gland, or a drug side effect, that problem needs to be treated first. If no underlying problem is found, the doctor may advise implanting a pacemaker.
Pacemaker - this device replaces the job of the atrioventricular node. A pacemaker is a small device that is placed under the skin of the chest or abdomen to help control abnormal heart rhythms; it uses electrical pulses to prompt the heart to beat at a normal rate.
Treatment for tachycardias (heartbeat is too fast)
Vagal maneuvers - certain maneuvers the patient can do himself/herself may stop an arrhythmia that starts above the lower half of the heart (SVY). This may involve the patient holding his/her breath and straining, coughing, or submerging the face in ice-cold water. The doctor, nurse or a specialized physical therapist may suggest other maneuvers. These maneuvers affect the vagal nerves and often cause the heart rate to slow down.
Medications - these will not cure the patient, but are usually effective in reducing episodes of tachycardia as well as slowing the heart rate down when they occur. Anti-arrhythmic medications need to be taken correctly for best results and to avoid complications. In some cases, if the medications slow the heart down too much the patient may need to have a pacemaker.
Cardioversion - if the tachycardia starts in the atria (top half of the heart) and includes atrial fibrillation, the doctor may use an electric shock to reset the heart to its regular rhythm - this is called cardioversion. It is carried out externally; the patient is usually given a drug to relax. The procedure is painless.
Ablation therapy - ablation means "taking the disease away". One or more catheters go through blood vessels into the inner heart. They are placed in areas of the heart that are thought to be the sources of the arrhythmia. Electrodes at the ends of the catheter are heated. Sometimes the tips are cooled down and the problem tissue is frozen. A small spot of heart tissue is destroyed (ablated), creating an electrical block along the pathway that is causing the arrhythmia.
ICD (implantable cardioverter-defibrillator) - if the patient is at high risk of developing a very fast or quivering (fibrillating) heartbeat in the ventricles, an ICD may be implanted. There are also ICDs for atrial fibrillation (quivering in the upper half of the heart). The device is implanted near the left collarbone - electrode-tipped wires go from the ICD, through veins, to the heart. The ICD monitors the heart rhythm and paces the heart, just like a pacemaker as soon as it detects an abnormally slow rhythm. Experts say that an ICD is better at significantly reducing the risk of a fatal arrhythmia than medications.
Maze procedure - a series of surgical incisions are made in the atria (upper half of the heart). They then heal into scars in the atria that form boundaries that make the electrical impulses travel properly so that the heart beats efficiently. This is open-heart surgery and is usually used for patients who have not responded well enough to other treatments. Maze procedures have a good success rate.
Ventricular aneurysm surgery - if an aneurysm (bulge) in a blood vessel that leads to the heart is causing the arrhythmia and other treatments did not work, a surgeon may remove the aneurysm. This surgical procedure has a good success rate - it is sometimes used if the implanted ICD or catheter ablation did not work.
Coronary bypass surgery - a patient with frequent ventricular tachycardia who also has severe coronary artery disease may be advised to undergo coronary bypass surgery. Arteries or veins from elsewhere in the patient's body are grafted to the coronary arteries to bypass atherosclerotic narrowings and improve the blood supply to the coronary circulation supplying the heart muscle (myocardium).
 Symptoms of bradycardia include: (Sometimes there are no symptoms)
Symptoms of bradycardia include: (Sometimes there are no symptoms)