This is a relatively new and fast developing subspecialty of Orthopaedic and Trauma Surgery that encompasses a variety of procedures with the ultimate aim of helping improve the quality of life for patients with various complex and difficult lower limb problems, using often minimally invasive biological techniques of external fixation, quite often resulting in limb salvage. More commonly it provides the BIOLOGICAL solution to problems that would otherwise end up with joint replacement surgery at an early and relatively young age. Below are a few examples of limb reconstruction procedures.
 Nonunions: Some fractures refuse to heal for various reasons. In some cases, all that is needed is providing the correct biological environment for the fracture to heal. Modern techniques of external fixation provide such an environment with sufficient stability of the fracture at the same time allowing some micromotion which is now known to stimulate the fracture into healing. In more difficult cases, slow distraction techniques help stimulate the fracture to heal by what is called callus distraction. This is particularly useful for even more difficult cases with bone loss, where the defect can be made up by new bone formation at a different site. This is called bone transport. The beauty about modern external fixators is that we have full control over the position of the bone ends from the outside without resorting to repeated surgery. We can therefore stabilise, stimulate or lengthen the leg by stretching the callus. Nonunions: Some fractures refuse to heal for various reasons. In some cases, all that is needed is providing the correct biological environment for the fracture to heal. Modern techniques of external fixation provide such an environment with sufficient stability of the fracture at the same time allowing some micromotion which is now known to stimulate the fracture into healing. In more difficult cases, slow distraction techniques help stimulate the fracture to heal by what is called callus distraction. This is particularly useful for even more difficult cases with bone loss, where the defect can be made up by new bone formation at a different site. This is called bone transport. The beauty about modern external fixators is that we have full control over the position of the bone ends from the outside without resorting to repeated surgery. We can therefore stabilise, stimulate or lengthen the leg by stretching the callus.
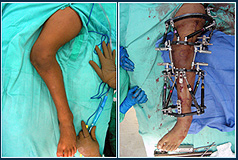
Deformity Correction: Deformities may be congenital or acquired usually as a result of fractures in the past which have healed in a bad position. This may have a variety of implications, commonly causing damage to joints over the years and resulting in early arthritis due to the malalignment.
• So what can be done?
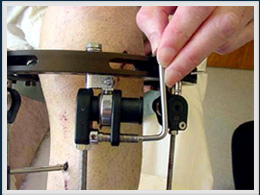
Well, an external fixator is applied to the leg and using a minimally invasive approach, usually through a tiny incision, an osteotomy (surgical division of the bone) is performed very carefully preserving the soft tissue attachments and blood supply to the area. The deformity can then be gradually corrected at home by the patient by turning a screw or nut on the external fixator until x-ray measurements show that the deformity is fully corrected. Again in the process, the gap created fills with the patients own new bone formation, unlike other open techniques where bone grafting is frequently necessary.
• So what then?
The hinges on the fixator are locked and the fracture allowed to heal usually by being stimulated by the micromotion produced by weight-bearing, which is encouraged at a very early phase with these techniques.
 • Do you mean the patient can walk with the fixator on? • Do you mean the patient can walk with the fixator on?
Of course, during the correction the patient is taught to walk with crutches taking minimal weight. Once the correction is complete, the patient is allowed to take increasing amounts of weight until full weight bearing long before full healing of the osteotomy. In fact this weight-bearing allied with the unique characteristics of the fixator stimulate healing of the fracture. Mobility in terms of joint motion and early weight-bearing is encouraged.
• Is it very painful?
Some pain is inevitable in the immediate postoperative period. This is however easily controlled with simple pain-killers for a short period. Subsequently very little in the way of analgesia is required. When the fixator is near a joint, it can cause some restriction of movement, but this is largely overcome by encouragement of active exercises very early on.
• Do I need another operation to have the fixator removed?
Not necessarily, this can often be done in the out-patients' clinic. No anaesthetic is required and the screws and wires are removed with little or no discomfort.
 • Sounds wonderful, any possible complications? • Sounds wonderful, any possible complications?
Yes. The most common problem is pin track infection. Of course it depends on the complexity of the case and how long the fixator remains in place. The vast majority of these are superficial which are treated either with simple pin-site care or with oral antibiotics for a few days. By and large this is regarded by most limb reconstruction surgeons and patients as an inevitable nuisance rather than a serious complication. It hardly ever leaves any residual problems.
• So what can be done?
Modern techniques allow gradual stretching of the leg using either an external fixator or intramedullary nail (a special lengthening nail). Following the operation, the patient performs the lengthening himself at a very slow rate of 1 mm per day, until the desired length is achieved. Then the lengthened area is allowed to heal until it is fully consolidated. |